Physical Therapy for FHL Tendonitis

FHL tendonitis is a common injury among ballet dancers that involves inflammation of the FHL tendon, often due to repetitive forceful movements or prolonged plantar flexion (toe pointing/dancing en pointe). The FHL tendon connects the calf muscle to the big toe, helping to flex the big toe and acting as a major stabilizer of the foot arch. Physical therapy can help dancers manage and address FHL tendonitis by strengthening the tendon and restoring range of motion and proper biomechanics in the foot and ankle complex through manual therapy, stretching, and therapeutic exercise.
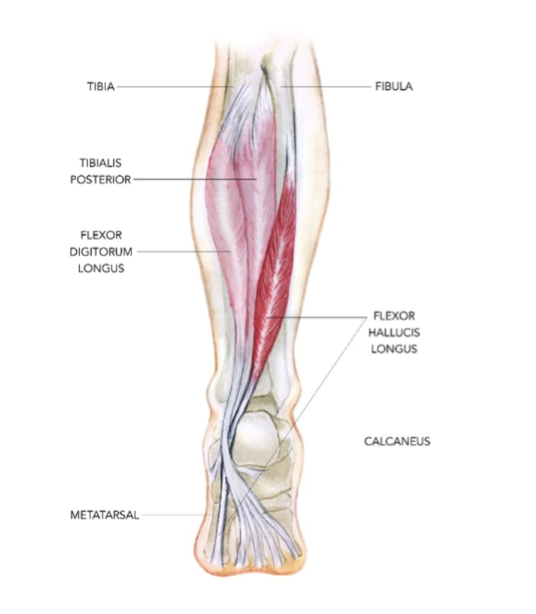
Anatomy of the FHL Tendon
The FHL tendon, or flexor hallucis longus tendon, is a strong fibrous cord that connects the calf muscle to the big toe, passing alongside the ankle. The FHL tendon helps to flex the big toe and allows you to stand on the tips of the toes, such as ballet dancers dancing en pointe. The FHL tendon also acts as a major stabilizer of the foot arch and helps control pronation and supination of the foot.
[Source]
What is FHL Tendonitis?
FHL tendonitis is a common injury among ballet dancers, particularly those who dance en pointe. It involves inflammation of the FHL tendon, commonly due to repetitive forceful movements or prolonged plantar flexion (toe pointing). FHL can also occur in runners and soccer, gymnastics, figure skating, cheerleading, and swimming athletes.
FHL tendonitis most often results from gradual wear and tear due to repetitive overuse of the tendon and nearby muscle groups. Repeatedly pushing off from the big toe can irritate the tendon and cause inflammation. Dancing en pointe involves excessive plantarflexion of the ankle, which places the FHL tendon under significant strain.
Dancers can be more prone to FHL tendonitis due to ligamentous laxity, poor en pointe technique, or excessive pronation of the foot. Excessive pronation can occur due to weakness in the hip, lower extremity, and core musculature, which can cause changes in foot posture, mechanics, and control, placing stress on the FHL tendon. Excessive eversion and pronation of the foot can occur when a dancer forces turnout or does not have enough hip strength to control turnout.
Other factors that contribute to FHL tendonitis include inadequate warmups or muscle weaknesses, incorrect technique, inadequate rehabilitation after an earlier injury, poor foot mechanics like flat feet, or limited flexibility.
Symptoms of FHL tendonitis can include:
Pain develops gradually over time, extending from inside the ankle down to the big toe
Pain worsens when the dancer pushes off from their toes
Swelling in the ankle
Clicking sensation or sound in the ankle, especially when flexing the big toe
Stiffness after resting the affected leg
Pain when touching the FHL tendon along its course from the calf to the big toe
Physical Therapy for FHL Tendonitis
Physical therapy can help dancers manage and address FHL tendonitis by strengthening the tendon and restoring range of motion and proper biomechanics in the foot and ankle complex through manual therapy, stretching, and therapeutic exercise. The therapist also helps the dancer modify and correct movements to minimize the loading and stress placed on the FHL tendon. The primary treatment for FHL tendonitis is conservative management through physical therapy and activity modification.
Physical therapy treatment for FHL tendonitis can include:
Rest and activity modification to decrease inflammation and swelling of the tendon
Use of ice to reduce inflammation and minimize pain
Compression and elevation of the ankle to stabilize the joint and reduce swelling
Manual therapy involving joint and soft tissue mobilizations of the foot and ankle to restore range of motion and mobility and manage pain
Stretching exercises of the calf, ankle, and foot muscles to alleviate muscle tightness
Targeted strengthening of the core, hip, leg, ankle, and foot musculature to address muscle imbalances or weaknesses that contribute to FHL tendonitis
Foot mechanic and dance technique instruction to reduce winging or rolling in when performing certain movements which can stress the FHL tendon as well as modifying turnout positions, en pointe, and jumps to reduce stress on the tendon
Return to dance progression involving gradual loading of the tendon to prepare for the demands of dance
Home exercise plan for long-term maintenance and re-injury prevention
Several case studies have shown that physical therapy management of FHL tendonitis is effective in restoring function and mobility in the ankle and foot. In one case, a 23-year-old athletic male presented with a 14-month history of left foot medial arch pain and was diagnosed with FHL tendonitis. His course of treatment included manual therapy, stretching, strengthening exercises, soft-tissue mobilization, and activity modification. Following treatment, the athlete experienced a significant reduction in pain and was able to return to running without exacerbation of symptoms.
In another case study of a young pre-professional ballet dancer with FHL tendonitis, the condition was successfully managed using conservative physical therapy treatment, which involved soft tissue and joint mobilizations, kinesiology taping, and rehabilitative exercises over 4 months of treatment. After treatment, the dancer reported a significant decrease in pain and improvement in lower extremity function [notable improvements in hip strength and mobility and improved endurance and strength while dancing en pointe] as well as a full return to her dance training.
Are you a dancer experiencing FHL tendonitis and foot and ankle pain? Work with a physical therapist to address pain and restore function and strength in your foot and ankle for a safe return to dance!